Publication highlighted: Lin et al., Microchemical Journal 220 (2026) 116569. doi:10.1016/j.microc.2025.116569
Executive summary
Next-generation sequencing (NGS)-based NIPT offers excellent clinical performance, but many laboratories face barriers in cost, workflow complexity, and turnaround time. In a recent Microchemical Journal study, Lin and colleagues report a multiplex droplet digital PCR NIPT (dPCR-NIPT) strategy that performs two clinically decisive tasks in one assay: (i) calling common fetal aneuploidies (T21/T18/T13) and (ii) quantifying fetal fraction from maternal plasma cell-free DNA (cfDNA). The study reports analytical sensitivity down to 5% fetal fraction with as little as 5 ng cfDNA input, and full concordance with an NGS-NIPT comparator in a 180-sample clinical set.
1 | Clinical need: why an integrated assay matters
NIPT is built on the detection of fetal-derived cfDNA circulating in maternal plasma. (2) A core operational limitation of many NGS-based workflows is that fetal fraction assessment and aneuploidy calling often rely on separate computational steps and quality thresholds, which can prolong reporting and increase no-call rates in low-fetal-fraction cases. An integrated digital PCR design can couple fetal fraction quantification with the aneuploidy call in the same analytical framework, improving interpretability of borderline results.
2 | Technical approach: two measurement engines running in parallel
A. Aneuploidy detection by digital counting
The assay quantifies chromosome 21, 18 and 13 targets using multiplexed reactions and converts droplet counts into chromosome ratios (R values) and Z-scores for classification, using a Z-score threshold of ±3 in the study. (1) A notable design principle reported is that increasing the number of primer pairs increases measurable copy number and stabilizes ratio precision once sufficient counts are reached. (1)
B. Fetal fraction quantification using methylation-informed cfDNA measurement
The authors quantify fetal fraction using differentially methylated regions (DMRs) and methylation-sensitive restriction enzymes (HhaI and HpaII) to preferentially suppress maternal signals while preserving fetal hypermethylated fragments, followed by multiplex droplet dPCR measurement. (1) This design enables fetal-fraction estimation independent of fetal sex, while still allowing benchmarking against Y-chromosome-based approaches when applicable. (1)
Figure 2. Illustrative 1D amplitude plot showing separation of negative and positive droplets
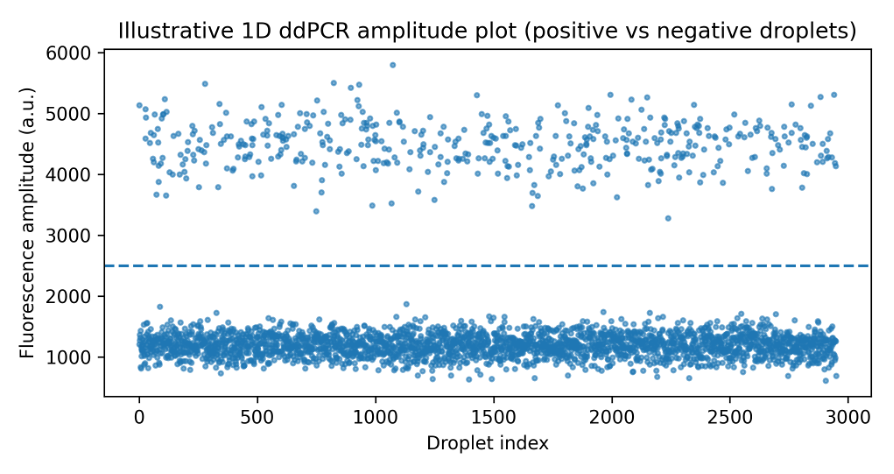
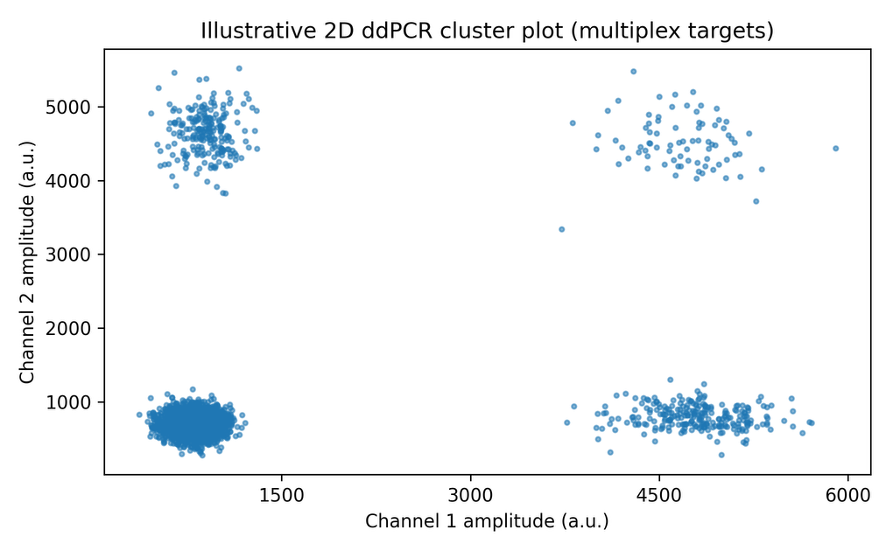
Figure 3. Illustrative 2D cluster plot for multiplex droplet dPCR
3 | Why digital PCR: absolute quantification and decision-grade statistics
A practical advantage of droplet digital PCR is absolute quantification: partitioning the reaction into thousands of droplets enables direct estimation of target molecule counts without standard curves, improving robustness for small effect sizes and low-abundance signals. (5) This is central to NIPT by counting, where the expected trisomy shift can be only a few percentage points depending on fetal fraction. Earlier feasibility modeling showed why large numbers of counts are needed for strong statistical confidence, motivating high-partition, high-multiplex designs. (3) A proof-of-concept ddPCR NIPT study also reported trisomy detection at approximately 5% trisomic DNA fractions, aligning with the analytical limit reported in Lin et al. (4) (1)
Figure 4. Illustrative relationship between fetal fraction and Z-score separation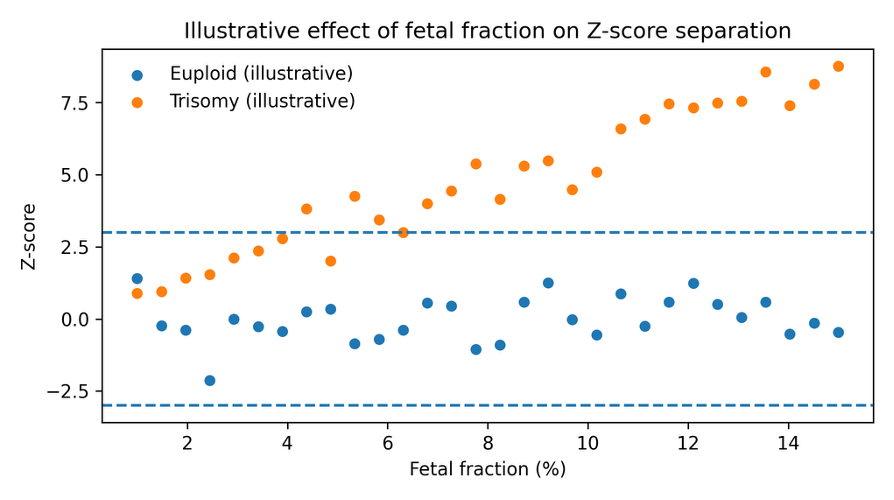
4 | Workflow implications: faster reporting with an all-in-one droplet dPCR platform
In the highlighted study, the multiplex dPCR-NIPT was implemented on an all-in-one droplet digital PCR platform that automates partitioning, PCR amplification, fluorescence detection, and downstream analysis within a single workflow. (1) The authors describe a total processing time on the order of hours for dPCR compared with multi-day timelines commonly associated with NGS-NIPT workflows in their setting. (1)
For laboratories evaluating droplet digital PCR for high-consequence quantification workflows, this paper demonstrates how automation, partition count, and multiplex design can combine to support clinically meaningful turnaround time and analytical performance. (1)
5 | Practical limitations and adoption considerations
Digital PCR changes the economics and speed profile, but it also changes what you can and cannot see. If you are considering dPCR-NIPT for routine use, the key questions to stress-test are:
Scope: targeted assays typically focus on common trisomies (and a limited set of loci), whereas NGS can support genome-wide screening and some microdeletion workflows, depending on the pipeline.
Edge cases: low fetal fraction, confined placental mosaicism, maternal copy-number variation, and vanishing twin scenarios can still complicate interpretation in any cfDNA-based screening workflow.
Counting statistics: achieving tight Z-score separation requires sufficient droplet counts and balanced multiplex efficiency; assay design and QC thresholds are therefore non-negotiable.
Clinical governance: as with all NIPT approaches, results are screening outputs and should be confirmed by diagnostic testing pathways consistent with local clinical practice.
6 | References
7 | Learn More
Sniper DQ24 Digital PCR System: Explore on Darwin Science
Gene Expression Analysis with DQ24: How it enables absolute quantification
#DigitalPCR #ddPCR #NIPT #CellFreeDNA #FetalFraction #Trisomy21 #Trisomy18 #Trisomy13 #MolecularDiagnostics #PrenatalScreening #AbsoluteQuantification